

Coronary artery calcium scoring
Coronary artery calcium scoring
Coronary artery calcium scoring is a technique which measures the amount of calcium in the coronary arteries using ECG-gated non-contrast computed tomography (CT) scan of the heart.
A calcium score provides a quantitative assessment of calcified atheroma burden, helping to risk stratify asymptomatic patients. This can help guide statin therapy and allow provision of advice regarding coronary risk modification. A calcium score of zero essentially excludes coronary artery disease in patients over the age of 45.
Calcium scoring provides a surrogate measure of total atherosclerotic plaque burden, but it is not specific for luminal obstruction. As CAC and plaque burden increase, there is proportionate rise in the risk of cardiovascular disease (CVD) events.
Advantages
Calcium scoring can help predict the risk of a future cardiac event in an asymptomatic individual in the setting of primary prevention.
It can be considered ‘individualised coronary risk scoring’ and allows classification of patients into either lower risk, with potential cost-savings in minimising therapy, or into higher risk groups where appropriate therapies may improve outcomes.
The CT scan acquisition is relatively quick (less than 10 seconds), has low radiation exposure (~ 1mSv) and does not require intravenous contrast or special preparation.
Clinical Indications
Coronary artery calcium scores are of most use in those patients at intermediate risk for cardiovascular disease, where the result will either lower or raise the risk profile and provide a change in management (absolute 10-year cardiovascular risk of 10-20%^) who are asymptomatic, do not have known coronary artery disease and are aged 45 – 75 years.
It may also be considered for lower risk patients (absolute 10-year cardiovascular risk 6-10%^) particularly in those where traditionally risk scores under estimate risk e.g. especially in context of family history of premature CVD and possibly in patients with diabetes aged 40 to 60 years old. (Cardiac Society of Australia & New Zealand)
^ Framingham Risk Score
When is calcium scoring NOT recommended?
Calcium scoring is not recommended for patients who are:
- At very low risk (<5% absolute 10 year risk); or,
- High risk (>20% absolute 10 year risk) - as testing is unlikely to alter the recommended management. This includes some patients who are automatically considered to be high risk (e.g. diabetics over 60 years old or diabetics with albuminuria, chronic kidney disease (eGFR < 45 mL/min), BP > 180/110, familial hypercholesterolaemia and cholesterol > 7.5 mmol/L) and therefore should be managed aggressively with optimal medical therapy; or
- Symptomatic or previously documented coronary artery disease.
In the assessment of symptomatic patients, it is recommended that coronary CTA, functional testing or invasive coronary angiography be used as appropriate.
Management recommendations based on calcium scoring
Optimal diet and lifestyle measures are encouraged in all risk groups and form the basis of primary prevention strategies.
Patients with moderately-high or high risk based on calcium score are recommended to receive preventative medical therapy such as aspirin and statins.
The evidence for pharmacotherapy is less robust in patients at intermediate levels of CAC 100-400, with modest benefit for aspirin use; though statins maybe reasonable if they are above 75th centile.
Aspirin and statins are generally not recommended in patients with CAC < 100.
Should we repeat the test?
One of the most common questions faced by clinicians and patients after an initial calcium score is if or when another is needed. Currently there are no studies which show a regression of calcium scores on subsequent scans. Therefore, the result can either remain the same or more likely worsen with time.
In patients with a calcium score of 0, a repeat calcium score may be considered in 5 years but not sooner.
In patients with positive calcium score, an annual increase in calcium score of >15% or annual increase of calcium score >100 units are predictive of future myocardial infarction and mortality.
Reference: The Cardiac Society of Australia and New Zealand, Coronary Artery Calcium Scoring Position Statement, May 2017.
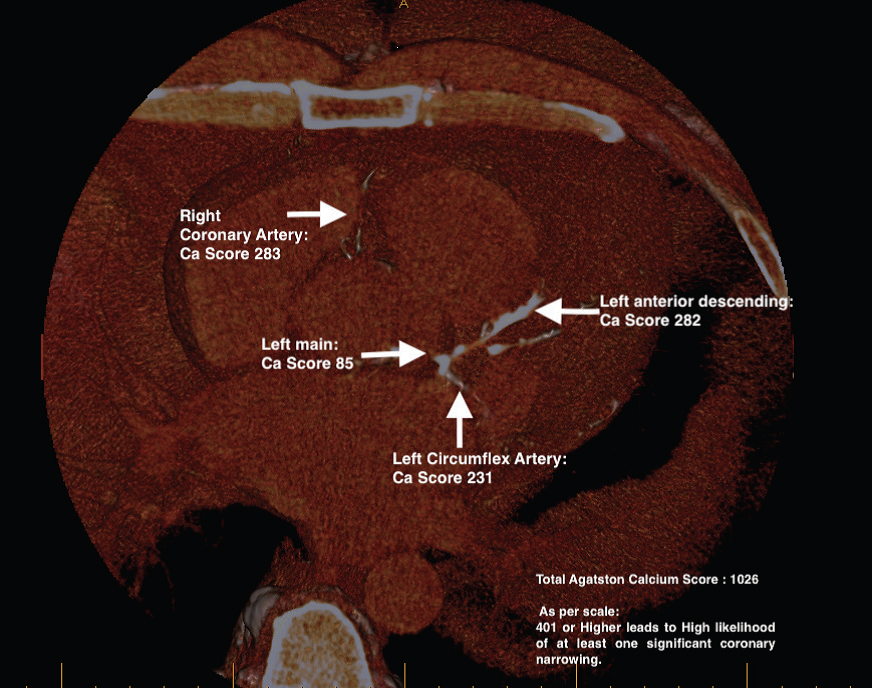
57 year old male with recent onset of Atrial Fibrillation showing an intermediate risk profile.
Download the coronary artery calcium scoring information sheet here.